Unexpected "Adventure" in Kilimanjaro |
| After the vasectomy mission in Kisumu, Kenya, the plan was to travel from Kisumu to Kilimanjaro via Nairobi on Sunday August 4 and spend the night at a hotel in Moshi, Tanzania, about 40 km from JRO (Kilimanjaro International Airport). There, we (Doug, Alison, Ramon, and Alexa) would join the non-mission members of our trekking group (Maryann,Steve, Stefan, William, Juan, Gail, and Christine) and prepare for our 8-day trek up the Lemosho Route with Zara Tours. |
 |
 |
| In Nairobi, the Kenya Airways planes were lined up in rows ... | ... as we tranferred to a Precision Air flight to JRO at about 6 PM. |
 |
 |
| We were a happy group, | excited about seeing the big mountain lit by the setting sun. |
 |
 |
| We were not disappointed. It was as if the clouds had lowered, | but the mountain, at 19,341 feet was even higher than our cruising altitude of 17,000 feet. |
| By the time we secured our luggage and linked up with our driver from Zara, it was after dark. We piled into the back of the van and headed on initially-empty roads toward Moshi. We never really thought about seat belts. Most of the transport vehicles in Africa either don't have back seat belts or they are lost under the seats. And we had spent most of our transport time in Kisumu crammed in the back seats and storage areas of SUVs. Traffic got heavier. As a motorcyclist with passenger attempted to pass us and 3 other vehicles, our driver "tsk"ed his recklessness under his breath. Suddenly, an oncoming vehicle appeared, slammed into the motorcycle, and was thrown out of control into our lane. We hit him head-on. Alison was on the right side behind the driver (they drive on the left in Kenya, as in Britian), next to German geologist Johannes, who was planning to join our group on the Lemosho Route. I was behind her in the third row, beside Ramon, who was behind Johannes; and Alexa had the 4th row of seats to herself, sitting a bit left behind Ramon. As our bodies flew forward with the impact, I fleetingly thought that this was how it was going to end. But in the errie silence that followed the crash, everyone was moving, and only Alison was calling out in panic and pain. | |
 |
 |
| Ours was the vehicle on the right. | We really don't know why any of us survived. |
| We all uttered our share of expletives that are bleeped on public media. But that told us that at least we were all alive. Alison had slammed into the back of the driver's seat and knew right away that her left wrist/arm was broken. I had been thrown forward and a bit to the left. Why Johannes did not go through the windshield, none of us can explain, unless the angle of the impact threw him a little left into the back of the front passenger seat. As you can see, there is no evidence in the photos of a deflated airbag, but perhaps there was one. I tried to calm Alison and escort her out of the van as she supported her left arm. Blood was streaming from cuts around her right eye, but she could see. The scar over her right patella from her ACL repair in January had ripped open. The rest of us were bruised, but nothing serious. | |
 |
 |
| Alison's wrist was deformed as we sat on the side of the road in shock. Johnannes offered a headlight so that I could examine Alison, and others whipped out cell-phone flashlights. People began to appear from out of the dark night. A car pulled up and its driver, who we later learned had been a guide for Zara tours, brandished a gun, and warned the locals to stay away. Apparently, they loot accident vehicles before offering any help, and all of our valuables were in that van. Shortly thereafter, another Zara Tours van arrived on its way from the airport. Ramon and I had both lost our eyeglasses, but I thought of and secured my computer immediately and the other 4 (now including Johannes) got their personal packs. Our pistol-wielding good samaritan offered to take us to the hospital in his sedan while the second Zara van took our dufflebags and the NSVI suitcases full of valuable surgical supplies to the hotel. | On arrival at the Kilimanjaro Christian Medical Center,
Alison's face was washed and crudely bandaged. Her knee was
dressed and a sling was improvised out of gauze. Arrangements
were made for an x-ray and orthopedic consultation. Much to our pleasant surprise, one of the Zara Tours workers arrived and proudly presented to Ramon and me ... our eyeglasses, slightly bent but otherwise intact. |
 |
 |
| We waited at least 2 hours for the X-ray, but the staff of Zara Tours, led by Rashid Adam, brother of the owner, stayed with us the whole time. Adam would take me periodically to the cashier to make payments for drugs, supplies, and services, but it never mounted to more than about $150 total. He said it was important to slip the staff a few dollars to move the process along, so I went through a half-dozen $5-$20 bills and people seemed happy. He also showed me to a bathroom with just a hole and no toilet paper. An assistant found a near-empty bag of wetwipes, which sufficed. There was no hand soap, but no matter because the sink faucet was dry. | The break was clean. The orthopedic resident arrived when Alison was in X-ray. She was from Zimbabwe, and had gone to medical school 30 km outside Moscow, so she was fluent in English, Russian, Swahili, and her local tribal language. She seemed very sure of herself and she inspired confidence. She indicated that Alison would need closed reduction and a splint. It would hurt, but she could administer IV Valium. |
 |
 |
| Alison had a deep slit on her eyebrow, an avulsion of skin with a dead skin tag beneath her eye, additional smaller cuts in her eyelids, and loss of some upper and lower eyelashes. | While we waited for the closed reduction, I managed to clean and dress the gash under the eye, but knew it would need more. Forced smiles belie the heartbreak of knowing she would not be able to climb. |
| While all of this was happening, I began to notice increasing tenderness of my left rib cage, front and back, and soon I was convinced that I had broken a few ribs. | |
 |
 |
| After the ortho resident probed Alison's right antecubital fossa with a large angiocath for a vein, obviously without success, Nurse Nelly started an IV in the intern's vein. | 10 mg of IV Valium made her feel much better. |
 |
 |
| The ortho resident recruited a burly GP to help with the closed reduction. Torture for 5-10 seconds, then relief. | The arm was wrapped and a plaster split was applied. |
 |
 |
| Trying to make the best of the situation, Alison stayed cheery, which amused the hospital staff. She was an absolute trooper. | A general practioner came in after her arm was treated to address her knee wound. His attire included a Versace sport coat, darkly tinted glasses (apparently light sensitive?). |
 |
 |
| The scar from her ACL surgery had ripped open and one could feel the patella in the depths of the hole. I was concerned about infection and slipped Alison a quick 500 mg Keflex from the stash of pills in my waist pouch. | The doctor debrided the necrotic tissue from the wound margins, sutured the deeper layers with heavy-guage absorbable suture, then approximated the skin with another two heavy gauge sutures of silk on a tapered (not cutting) needle. |
| The tapered needle could barely get through the tough skin, and he fumbled a bit because he did not have a needle driver, only an oversized Kelly clamp. | |
 |
 |
| Stitching in progress, no sterile fenestrated drape, no procedure light. | Finished product - pretty rough stuff. |
 |
 |
| We removed the temporary dressings previously applied to the face and were disappointed to find wounds deeper than we expected. We debrided the flap of dead skin under they eye and I asked for some fine nylon. All they could offer was the same heavy-guage silk. No way. Not in MY daughter's face. Adam had some Steri-Strips in his first aid kit, and I did the best I could to approximate the skin margins with that. | We arrived at the hotel at 3:30 AM. By now, my ribs were
really bothering me and I took a Tylox to help me get some
sleep. Next morning, we met the boys and the rest of the gang. No way could Alison climb with the broken arm and the face and eyelid injuries that needed a good plasticsurgeon. And I was in bad shape with rib pain made worse by any deep breathing. |
| So we determined to return to the USA ASAP to get the care she needed. Little did we know what was in store for me. | |
 |
 |
| Gear and hikers were loaded onto and into buses ... | |
 |
 |
| ... and we said our teary goodbyes. | |
 |
 |
| We had a hearty breakfast in the eating area formerly crowded with hikers from all over the world. Zara Tours called Ethiopian Airlines to arrange for the 5:45 PM flight back to Addis Ababa that day, and we packed our gear. When the van arrived to take us to the airport, a van nearly identical to the one in which we had nearly been killed, we made sure that seat belts were available and fastened. | |
 |
 |
| Once again, we traveled the lonely road that connects Moshi to Kilimanjaro. | Stomachs in knots, we were taken aback by the crazy driving we saw as big vehicles were passing other cars with very little clearance. |
 |
 |
| We stopped at the accident site to see if we could find any debris to piece together the chain of events a little better. The German geologist, Johannes, and Alison observed the evidence of the fateful night. | We came across a side rearview mirror, probably from the motorcycle, as well as other remnants from the crash vehicles, including a near-intact windshield. |
 |
 |
| Business Class travel permitted use of the comfortable lounge in the Kilimanjaro Airport. | |
 |
 |
| A Tusker for Alison and South African Liqueur reduced the physical and emotional pain. | Leaving Kilimanjaro. |
 |
 |
| The pilot had a friend on board and took us very close ... | ... and partway around the mountain that we had hoped to feel with our feet as well as our eyes. |
 |
 |
| Exhausted. | |
 |
 |
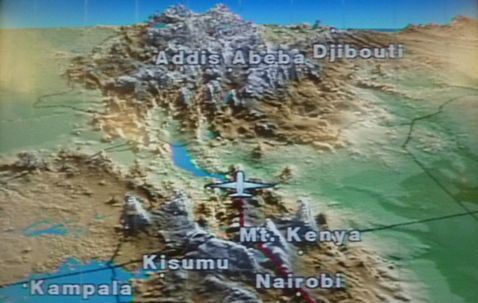
| Skymap made the Great Rift geography look very exciting. | Ethiopia has some really cool landscapes and fauna, but we felt more inclined to limit our viewing of them to TV, unless we could be guaranteed freedom from illness or injury. |
 |
|
|
After stopping for fuel in Rome, I anticipated a good rest
across the Atlantic, but the left back and left upper quadrant
pain became progressively worse and it was difficult to get
comfortable. In Washington's Dulles Airport, Delta allowed us to catch a flight to Tampa via Atlanta without a fee for the change from August 14 to August 6. But by the time we arrived in Atlanta, walking was even more difficult, so Delta offered a wheelchair for the transfer from Concourse A to E. By this time, I was concerned that I might have more than fractured ribs, perhaps delayed presentation of a ruptured spleen. My Primary Care Doctor in Tampa, also a gastroenterologist, suggested that I go to the nearest emergency room, as going into shock at 30,000 feet is not good.  |
 |
| So Delta called EMS and I was taken by ambulance to Atlanta Medical Center. Both airport EMS and the ambulance staff were extremely professional and caring. My BP was 170/105, but better than being low. | |
 |
Any movement was painful, but this was exaggerated by the
anxiety that I might have something injured INSIDE. When still,
I was fine and my blood count was normal ... relief. During typically long ER waits, we worked on this web page and updated family members by phone. Then I had a CT scan of the chest and abdomen. All I had was broken ribs on the left side. We were cleared to return to Tampa, left the ER at 10 PM, and caught an 11:07 PM flight. According to periodic text messages, the rest of our climbing group are apparently making good progress. My wife Maryann, my cousin Steve and his 2 sons, their friends Juan, Gail, and Christine; and NSVI President 76-year-old Ramon Suarez and his 16-year-old grand-daughter Alexa. On the Summit, they will raise a banner for World Vasectomy Day, a ceremony that Alison and I had hoped to attend. We feel, however, very lucky just to be alive. |
When not out of alignment, rib fractures can be difficult to
find, but this one seems rather obvious.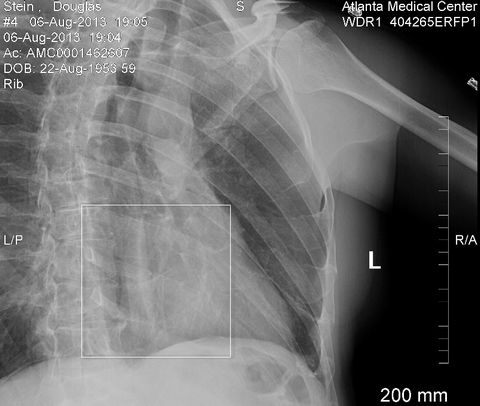 |
 |
| Back in Tampa, I ordered films of Alison's arm for presentation to her orthopedic surgeon. | |
 |
 |
| Alignment is not perfect, but I was told that closed reductions involve a bit of luck, and no ground has been lost because healing does not commence for a few weeks. After a curbside conference, he indicated that the best plan for optimal alignment and minimal cast time would be a plate and screws, usually not palpable or visible from the outside after healing. | |
 |
 |
| At the office of her ophthalmologist/eyelid-specialist, Alison's dressings were removed and her wounds closely examined, directly ... | |
 |
 |
| ... and with magnification. She may need a small skin graft from behind the ear to the wound beneath her eye, | but photos of similarly treated patients hold the promise for minimal scarring. |
| What a pleasure to be back to excellent and well-equipped American surgeons! | |
 |
 |
| On Friday, August 10, Day 5 for Ramon and the other Kilimanjaro Hikers, | I drove Alison to the orthopedic clinic. |
| Her Tanzanian splint was digging into her swollen left hand and causing blisters behind her arm. We did not want to wait until her scheduled Wednesday surgery to address those problems. The ortho techs got a hearty chuckle out of the fact that her arm had been wrapped in toilet paper of paper towels before the Tanzanian splint had been applied. | |
 |
 |
| They applied a REAL First-World-Quality splint. Not pleasant to have a broken arm manipulated, but what a relief when it was done. | |
 |
 |
| Then we cruised across Tampa Bay to the eye surgery center in St. Petersburg, where she underwent repair of eyelid lacerations and application of a skin graft from behind her ear to the avulsion beneath her eye. Without a skin graft, the contracted cheek wound would have resulted in a droopy lower eyelid. No photos were allowed in the center, but her dressings are now smaller. | |
 |
|
| What a treat to get a photo of Maryann (on Kili
at Camp 5) during Alison's busy doctor day. The next four days were a waiting game. Despite the new splint, Alison had periodic lightning bolts of pain where the bone was broken. During those days, we were pleased to learn that our Kilimanjaro Team ultimately made it to the summit. |
|
 |
 |
| Finally the day of surgery arrived. The anesthesiologist used ultrasound to guide a needle into the area of her brachial nerve just above her collar bone. Her arm became numb and she was wheeled into a huge modern operating room, luxury compared to the facilities in Tanzania. | |
 |
 |
| Alison snoozed, but was always easily arousable ... | ... while Dr. Gray exposed her broken bone. |
He fitted the margins perfectly back into place, laid a
plate into position, drilled a few holes, and screwed the plate
onto the bone. |
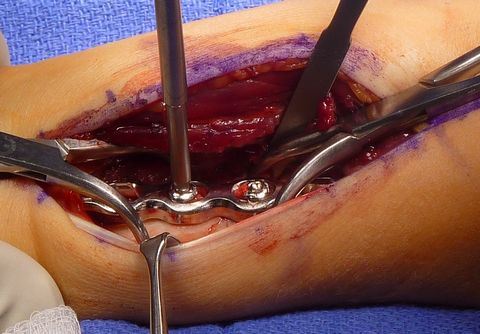 |
 Dr. Gray used flouroscopy to confirm that the fracture margins were in perfect alignment, secured by three screws proximal and three screws distal to the fracture. |
 |
| In fact, one view (below right) shows such tight apposition and such perfect alignment, that one cannot even see the fracture margins. | |
 |
 |
 |
 Dr. Gray checked all of her wrist bones (left), applied a new plaster splint and a new sling, and Alison's I.V. line was removed about 2.5 hours after it was inserted. What a great surgeon and professional team! |
 |
On the way home, we stopped back at Dr. Older's office.
Alison's skin graft dressing was removed and all wounds checked. She was cleared to discontinue all dressings and leave the graft open to the air except for just a coating of antibiotic ointment. She will keep her arm elevated and iced for a few days, and she should be free of a cast or splint in two weeks. We would rather have climbed Kilimanjaro, but we've tried to make the most of our own little adventure.  |
| On August 28, nineteen days after her facial surgery on August 9, Alison's skin graft looked good. The sutures (left photo 2 days after the procedure) ... | |
 |
...had all fallen out by 19 days. |
 The eyelid injuries are healing well, the brow scar should be hidden by, well, brow; and we hope the new skin and graft of her cheek injury will lighten and blend. |
 |