Sperm Recovery Data:*
The single most important factor in whether a vasectomy reversal attempt will be successful is the interval in time (years) between vasectomy and vasectomy reversal. We keep all of our data on an Access database which we can use to answer certain "queries," and which can be exported to an Excel file and used to prepare the graphs you see below. Updated data is published to this web page every 1-2 months. This allows any reversal candidate the opportunity to determine the likelihood of sperm recovery and pregnancy with a reversal in this office. Data published by other offices or institutions is of little use to the couple trying to assess a particular office. Vasectomy reversal is a gamble, and success rates and fees vary from office to office, so all the evaluating couple can do is determine where they may obtain the most value for their investment. For example, if the candidate's interval is say 4-6 years and one office has rates of 93% (sperm recovery) and 70% (pregnancy) for a fee of $5000, and another office offers convincing rates of 97% and 73% for $7000, then only the couple can decide whether the increment in higher success is worth the fee differential.
Because the interval in time (years) between vasectomy and vasectomy reversal is so important, the first graph below shows the relative numbers of men at each interval who have experienced sperm recovery (a return of sperm to the semen; blue columns) vs. no sperm recovery (red columns). The height of the columns is not the measure of success, but just the number of patients at each interval. The measure of success at each interval is the height of the blue column divided by the combined heights of the blue and red columns. Because of chance statistical variations (6 years just happens to be a lucky interval for us so far), we predict the likelihood of success at a certain interval by including the year before and the year after that interval. For example, to predict success at 6 years, we divide sperm recovery patients by total patients in the 5-7 year intervals.
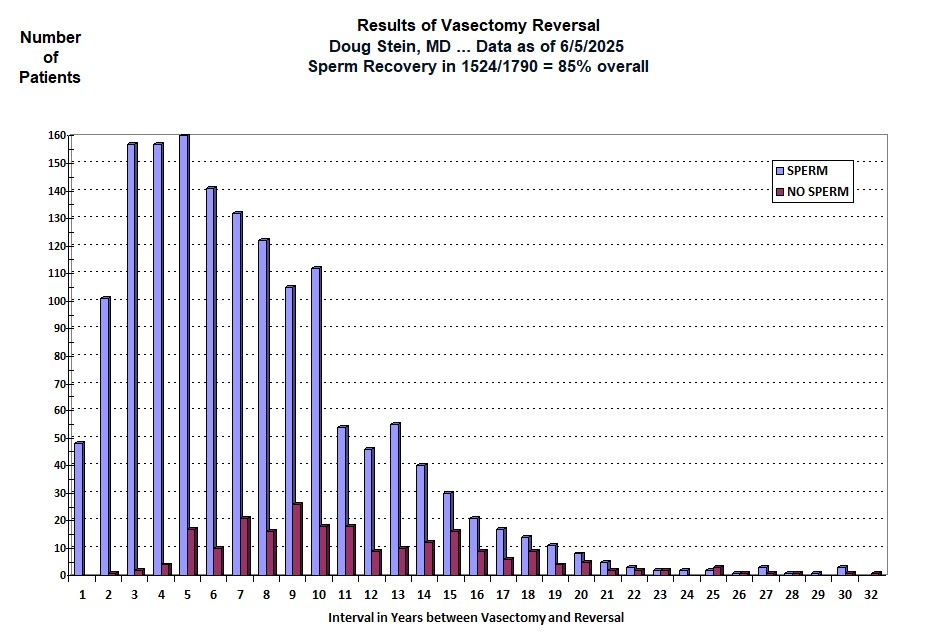
* - While Dr. Stein has performed over 2000 vasectomy reversals, the graph
above does not include unilateral (one-side) reversals, repeat reversals, and
patients who have not yet sent in semen samples. Data for unilateral and repeat
reversals is available on request.
** - ALSO IMPORTANT - Not all men represented by the red bars actually
underwent full vasectomy reversal. If, at the time of exploration, the
lower (testicular) end fluid is poor (creamy or thick, devoid of sperm, packed
with white blood cells) on both sides, connections are not performed, the ends
are simply dropped back into the scrotum, and the patient is charged no more
than his deposit. Yet, he is entered into this database as a "NO SPERM" and "NOT
PREGNANT". (It would be a waste of his money to perform connections when the
likelihood of success is minimal. That money would be better spent on other
options.)
Pregnancy Data:**
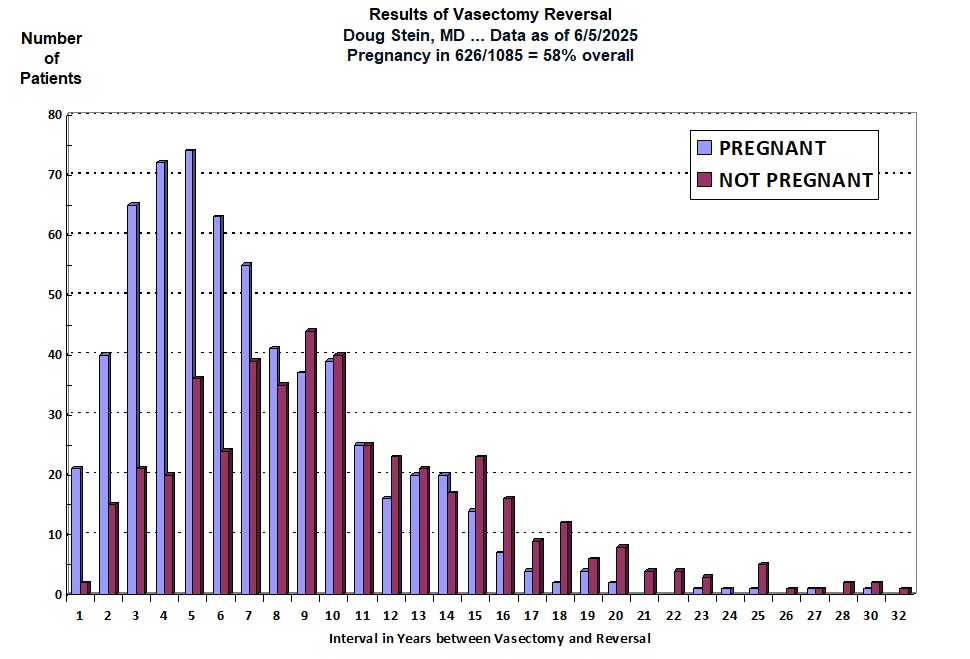
*** - Notice that the number of patients contributing to
the pregnancy database is considerably smaller than the number of patients contributing
to the sperm recovery database. Almost all patients send or bring in a semen sample
after reversal, so sperm recovery rates reflect the vast majority of patients who undergo
vasectomy reversal. Couples are added as "NO PREGNANCY" only if it has
been one year since the reversal and they have failed to conceive. When we have tried to call our
reversal patients who have recovered sperm, we've gotten all sorts of responses: "the number has been
disconnected or is no longer in service," "no-one by that name lives here," "we're separated," "my husband lost his job and money is tight right
now so I'm back on the pill," "I got a breast tumor and was told that pregnancy could stimulate my cancer if not fully
cured," "we didn't plan on getting pregnant right away, but had you do
the reversal to increase our likelihood of success in a few years," "my
father died and now I have to take care of my Alzheimer's mother and there is no
way I can take care of a baby and my invalid mother at the same time," and the list goes on.
Sometimes we learn about a pregnancy of which we were unaware and another
success is added to the data. Sometimes we learn that a couple has been trying
for more than a year but sperm density or motility is very low, and another
pregnancy failure is added to the data. Sometimes we learn that sperm density or
motility is low and the wife has endometriosis or had to have a tube and
ovary removed, and we are not sure whether entering the case as a pregnancy
failure is justified. Or a patient with a perfectly normal semen analysis gets
divorced 9 months after his reversal and his new partner has already had her
tubes tied: can't enter him as a pregnancy failure or success. Thus the many
reasons for the difference in the total numbers of patients included in the two graphs.
**** - Some couples fail to let us know about pregnancies until we call them. We
don't have the time or resources to call all patients with the above delay
factors periodically, so there may be more pregnancies than are
indicated in the graph above.
In addition, there are no set standards for reporting pregnancy rates. Some offices will enter a couple as a pregnancy failure only if pregnancy has not occurred within two years of the reversal, as opposed to one year as we do. This can make the data "look" better because those couples not pregnant by 18 months after the reversal would not be included in their data as pregnancy failures, whereas they would be included as pregnancy failures in our data. Pregnancy rates will look even better for those offices who do not include couples as pregnancy failures until three years after the reversal ... and so on.
One other point worth repeating ... If the lower end fluid on both sides is of such poor quality that vas-to-vas connections are not performed (because they would be unlikely to result in sperm return to the semen), the patient is entered into the database as a case of "NO SPERM" and "NOT PREGNANT" even though a vasectomy reversal was technically not performed. So many patients represented within the red columns did not have vasectomy reversals. But it is necessary to include them within the data presented to a couple BEFORE we know the quality of the man's lower end fluid.