Vasectomy is a safe, highly effective form of permanent birth control for men who are certain they do not want future pregnancies. At VasWeb, the procedure is performed in-office using local anesthesia, with a focus on comfort, efficiency, clear preparation, and follow-up testing.
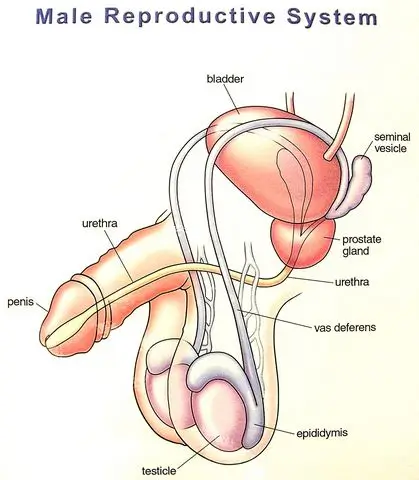
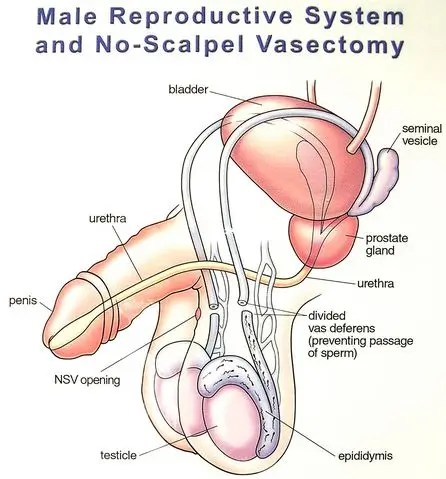
Sperm are made in the testicles and move through the epididymis, where they mature. From there, they travel through the vas deferens, the tubes that carry sperm toward the urethra, where they combine with the semen made by the prostate and seminal vesicles. During the procedure, these vas tubes are blocked so sperm can no longer enter the semen.
After the procedure, sperm may remain in the reproductive tract for several weeks. You must continue using other contraception until follow-up semen testing confirms that sperm are no longer present.
Sperm are still made by the testes after the procedure, but they can no longer pass through the vas deferens. White blood cells in the normal testicular circulation ingest, digest, and recycle the sperm that cannot exit the traditional way.
A vasectomy blocks sperm from entering semen, but most men notice:
Most men recover without serious problems after vasectomy. However, like any medical procedure, vasectomy has possible risks. These may include temporary soreness, swelling, bruising, infection, bleeding, sperm granuloma, chronic discomfort, or, rarely, failure of the procedure.
Some temporary discomfort and bruising, occasionally swelling and tenderness requiring the use of anti-inflammatory meds like ibuprofen. These effects are usually mild and improve with time, rest, and non-prescription medication.
Less common risks include infection; bleeding and development of a scrotal blood clot (very rarely requiring drainage in an operating room); development of a usually painless inflammatory nodule at the vasectomy site called a sperm granuloma; and ongoing periodic scrotal discomfort, occasionally severe enough to be described as Post Vasectomy Pain Syndrome and to require an operation for relief, as described in our consent for vasectomy HERE.
Vasectomy is highly effective, but it is not immediate. Sperm may remain in the tubes downstream from the vasectomy site after the procedure, so another form of contraception must be used until semen testing confirms that sperm have all been expelled and are no longer present.
Current evidence has not proven a link between vasectomy and long-term health problems such as cancer or cardiovascular disease. Patients with questions should discuss them with the doctor before the procedure.
There are no proven long-term health risks (neither cancer nor cardiovascular disease) associated with vasectomy, but since questions have been raised, they are addressed in our page of Frequently Asked Questions.
Consider the Alternatives to Vasectomy.
The risks of NOT having a vasectomy are all borne by the partners of men who choose to avoid vasectomy. And they are considerable!

Vasectomy should be treated as a permanent form of birth control. Although reversal may be possible, it does not always lead to pregnancy, so the decision should be made carefully and without pressure.
Vasectomy may be a good choice for men who are certain they do not want future pregnancies. Men in their 20s, men with fewer than two children, or anyone unsure about future family plans should take extra time to review all reversible birth control options before proceeding.
You should not have a vasectomy if you feel pressured, if your relationship or personal life is temporarily unstable, or if you have not fully considered alternatives. If you have never caused a pregnancy, sperm storage or additional testing may also be worth discussing before making a final decision.
If you have never caused a pregnancy, how do we know that you are fertile? 1% of men have no sperm in their semen (azoospermia) and a larger percentage have a low sperm count (oligospermia). The question is important for two reasons, which vary in importance depending on the age of the man considering vasectomy.
Young men (let's say, men under 35):
Young men who opt for vasectomy before fatherhood may be more likely so seek vasectomy reversal in the future than are men who choose vasectomy when they are in their 40's or 50's. If a young man who has never caused a pregnancy undergoes a vasectomy, then years later has a reversal that is "unsuccessful" (no sperm to the semen post-reversal), how do we know that he had sperm in his semen before his vasectomy? It would be nice to know this before your vasectomy in case you ever opt for a vasectomy reversal. Indeed, if you have no sperm in your semen, there is no reason for a vasectomy in the first place!
Older men (let's say, men over 35):
Nearly every man takes chances now and then by not using contraception despite the fact that he doesn't want to cause a pregnancy. Alcohol impairs one's judgment, and couples take more risks under its influence. If a man has reached his late 30's without ever causing a pregnancy, especially if he has failed to use contraception on a number of occasions, he must begin to wonder if he is fertile and whether he even needs a vasectomy.
For pre-vasectomy testing of semen, you have two options:
If you live close to our office in Tampa/Lutz, and you have completed our online registration, you may bring a semen sample to our office prior to your vasectomy. Bring it in a small container with a lid, such as a pill or vitamin bottle, baby food jar, etc. The sample should be 30 minutes to 4 hours old. Bring it M-F between 9 AM and 3:30 PM. There is no charge for that test.
Wherever you live, you may purchase a home test kit. Kits are available at some pharmacies, some retail outlets like Walmart, Amazon, Ebay, and some specialty companies. One is called SpermCheck Vasectomy. Search on "post-vasectomy semen test". If the test shows that your semen contains sperm, you will need a vasectomy to provide sterility.
If the pre-vasectomy office or store-bought test is negative, we will provide a lab request for a formal semen analysis to corroborate the simple office or home test with a more sensitive one. If the formal semen analysis confirms that there are no sperm in your semen, there is not much sense in having a vasectomy. We will suggest further tests if you would like to delve more deeply into why there are no sperm in your semen. For that, we charge no more than the $150 procedure deposit already paid when scheduling.
If you are not ready to schedule a vasectomy but would like to determine whether there are sperm in your semen, you may purchase a home test kit without a doctor's order (#2 above). For a formal semen analysis, you will need a doctor's order, and these tests are often covered by insurance.
So for various reasons, both younger and older men who have never caused a pregnancy should have their semen checked for sperm before undergoing vasectomy. From June 2012 (when we began this testing) to April 2019, 528 men who had never caused a pregnancy agreed to provide a semen specimen prior to vasectomy. Nineteen (19) of them had no sperm. Eight were on testosterone (known to stop sperm production in some men), and one had had chemotherapy and a bone marrow transplant. But that left 10 (of 519) men (2%) who had no sperm, yet no reason at all to doubt their own fertility potential. One man (age 44) with no sperm in his semen was delighted that he did not need a vasectomy, but wondered aloud how much money he had wasted on condoms all those years!
You may regret it. Men who have vasectomies when they are in their 20's, especially if they have had fewer than two children, may be the ones most likely to seek vasectomy reversal at a later date, often regretting their vasectomy decisions if their reversals are not successful.
You may change. Many men who think they will never want children when they are in their early 20's are delighted with fatherhood when they are in their 30's. You may be totally convinced now that you will never want children, but people change and you may have a much different outlook 10 years from now.
Women change. Similarly, women who have no desire for children when they are in their early 20's may have a much stronger desire when they are in their 30's and when many of their friends are having children of their own.
Relationships end. Since more than 50% of American marriages end in divorce, you may not be with the same partner ten years from now and a new partner may have a much stronger desire for children than your present partner does. So just because your present partner claims that she will never want children, her tune may change 10 years from now, or she may not even be your partner 10 years from now.
The philosophy of you and your partner with respect to abortion should be considered. If you are both not philosophically opposed to abortion, you have some back-up should other forms of contraception fail, and having a vasectomy now may not seem as critical to avoid an unintended pregnancy. But keep in mind that if she gets pregnant, the choice is hers.
Vasectomy should be considered a permanent and non-reversible procedure because vasectomy reversals are not always successful. So before having a vasectomy, know all of the other options ... HERE and HERE.
Young men should consider Sperm Storage. The companies who provide the service will send what you need directly to your home, you can collect the semen specimens in the privacy of your home, and you can mail them back to the company in the storage container provided. Imagine meeting a prospective partner years after your vasectomy. You fall very much in love with her, but you know that she will someday want children. You can tell her, "I have had a vasectomy", or you can say, "I have had a vasectomy, BUT I banked sperm for future use." Now, which do you think will sound better to her? In her eyes, either you did a foolish thing years ago, or you made a responsible decision with good foresight. In one case, you may lose the girl; in the other case, you win her heart. So sperm storage can be a very smart thing, well worth the investment.
Have you discussed your decision with your parents? If not, consider this: You're an adult, yes, but they helped you get there. How would you feel if your son came home one day and said that he had had a vasectomy? That he had done something to limit his future potential (to be a father) and to limit your own potential (to be a grandfather). How would you feel, after nurturing and guiding him for over two decades, if he did something to profoundly influence his future, but did not have the respect or courtesy to just tell you about it beforehand? As with many decisions in life, change the question from, "Should I tell my parents?" to "What can I do that I will never regret?" Would you ever regret not telling them? Possibly, especially if they are hurt as I, as a parent, would be. Would you ever regret telling them? Probably not. Having a vasectomy is still your decision, but at least you granted them the respect of letting them render an opinion. And if they succeed in discouraging you, because they know you better than any doctor does, you may one day thank them. If they don't succeed in discouraging you, they may split with you the cost of sperm storage and feel much better about your vasectomy in doing so.
All of this said, I recognize the fact that most of us know someone whose girlfriend said she could not get pregnant, or conveniently "forgot" to take her pills, or even poked pinholes in his condoms. And I recognize that our judgments can be impaired after a few drinks so that we are less inclined to cover up or pull out on time. Indeed some men perceive the risks of not getting a vasectomy to be greater than the risks of getting one. We must all be masters of our own destinies, and that is easier if we think through all of the implications, alternatives, and potential consequences of our decisions.
Parker had a vasectomy at age 18. His story is presented in the podcast HERE.
Some men would like to have a vasectomy even though their primary sexual partners (wives, fiancées, or long-term girlfriends) have already undergone bilateral tubal ligation, otherwise known as "BTL", "tubal", "tubal ligation", "tubes tied", or "female sterilization". There are a number of reasons for this:
The first reason is adequate justification for vasectomy, with the intended goal (avoidance of pregnancy with outside partners) being worth the risks of vasectomy.
The second reason is not MEDICALLY justifiable. That is, the risk of pregnancy after either vasectomy or tubal ligation is so low that the risk of either procedure is probably greater than the risk of pregnancy after either procedure. In the couple's minds, the two procedures may be SOCIALLY justifiable, but the second procedure does pose an unwarranted medical risk. My suggestion to such couples is that if they want to demonstrate their commitments to each other, an alternative method, such as simultaneous tattoos, would be less risky.
The third reason may be medically justifiable. One must compare the risks of vasectomy with the risk of pregnancy after tubal ligation. Data varies about both risks. See the table below.
Some men would like to have a vasectomy even though their primary sexual partners (wives, fiancées, or long-term girlfriends) have already undergone bilateral tubal ligation, otherwise known as "BTL", "tubal", "tubal ligation", "tubes tied", or "female sterilization". There are a number of reasons for this:
The first reason is adequate justification for vasectomy, with the intended goal (avoidance of pregnancy with outside partners) being worth the risks of vasectomy.
The second reason is not MEDICALLY justifiable. That is, the risk of pregnancy after either vasectomy or tubal ligation is so low that the risk of either procedure is probably greater than the risk of pregnancy after either procedure. In the couple's minds, the two procedures may be SOCIALLY justifiable, but the second procedure does pose an unwarranted medical risk. My suggestion to such couples is that if they want to demonstrate their commitments to each other, an alternative method, such as simultaneous tattoos, would be less risky.
The third reason may be medically justifiable. One must compare the risks of vasectomy with the risk of pregnancy after tubal ligation. Data varies about both risks. See the table below.
For those who want more detail: keep in mind that tubal ligation can be performed at three different "times" using one of a number of "techniques". Those "times" are:
At any "time" of tubal ligation, the procedure can be performed using one of various "<b>techniques</b>" to block the tubes. Here is a chart of the failure rates of those techniques:
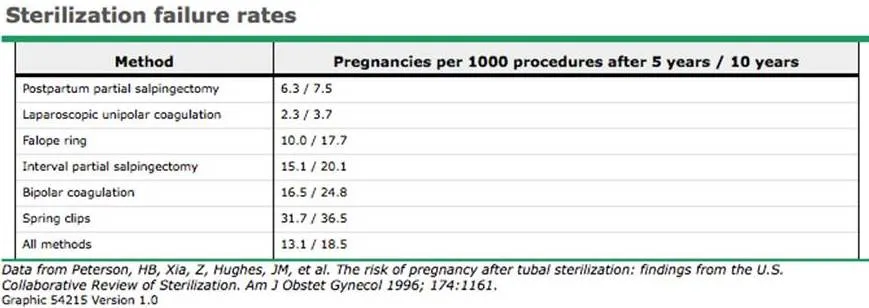
What this means is that, in the case of "Postpartum [after delivery] partial salpingectomy [removal of part of the tube]" (first line), 6.3 out of 1000 women, or 63 out of 10,000 women, will become pregnant within the first 5 years after this method of tubal blockage. That is fewer than 1%. In contrast, over 3% of women whose tubes are blocked with "spring clips" will become pregnant within the first 5 years after this method. Why would anyone use spring clips? Well, in the hands of some surgeons, spring clips may have a lower complication rate than other methods. The point is that tubal ligation failure rates may vary 10-fold with the technique used, but ALL methods of tubal ligation are very dependable compared with other forms of contraception. Birth control pills (BCPs), for example, have a failure rate of 3% EVERY YEAR. That is, of 100 women using BCPs, 3 will become pregnant every year. In contrast, of 100 women who have had tubals, 3 will become pregnant over 10 YEARS. So BTL is TEN TIMES more dependable than birth control pills. If a couple is concerned about a woman's risk of tubal ligation failure, and if the records of the tubal ligation method are available, and if a 0.37% failure risk vs. 3.65% failure risk over 10 years would influence their level of confidence in the BTL and their decision to opt for vasectomy, they could always review those records with her gynecologist to determine her personal risk of pregnancy.
At our Tampa/Lutz office (click for location and directions), we can usually see any candidate within two weeks.
Because there is so much information here in vasweb.com, especially with the online counseling video, we do not require preliminary consultation visits and most men opt for only one visit, during which we complete the consultation and procedure. If you would like to visit the office and meet Dr. Stein, Galante or Samplaski personally before deciding to proceed, we would be delighted to see you twice. (In fact, we prefer to consult with childless men in their 20's either in person or by telephone at least one week before their vasectomies to thoroughly discuss the issues in the Special Message above.) If the consultation and vasectomy are on separate days, either can be done on any weekday.
All scheduling is done by Heather and Sergio at 813-536-1430 between 9 AM & 4 PM M-F. They can also answer many insurance and logistical questions.
As you may have seen in the Florida map on our Home Page, we perform vasectomies at a number of locations in central Florida. A complete schedule with links to maps and information about these locations is in our SCHEDULE page.
You must register online before your visit, but when you arrive, you won't have to fill out all those papers like in many doctors' offices. The benefits are numerous and listed in our On-line Registration Page. Please do not hit SUBMIT more than once. Call our office (813-536-1430) M-F, 9-4 after submitting your registration to arrange a convenient appointment time.
A vasectomy is a minor in-office procedure that provides permanent birth control by preventing sperm from entering the semen. It does not affect the testicles, lower testosterone. Most men notice no change in sex drive, erections, or climax sensation.
The vasectomy procedure itself is usually brief, often around 15 minutes. The full appointment may take longer because it can include check-in, preparation, counseling confirmation, and post-procedure instructions. Many VasWeb patients complete consultation and procedure in one visit when appropriate.
Most patients feel pressure or mild discomfort rather than sharp pain because local anesthesia is used. Some soreness, swelling, or tenderness can occur afterward, but it is usually temporary. VasWeb provides preparation and aftercare instructions to help patients know what to expect before and after the procedure.
Many patients return to light daily activities within a few days, but heavy lifting, intense exercise, and sexual activity should wait until after the recommended recovery period. Some mild soreness or swelling can happen early on. Patients should follow VasWeb’s aftercare instructions and contact the office with concerns.
You should not stop using other birth control immediately after a vasectomy. Sperm can remain in the reproductive tract for weeks after the procedure. Another form of contraception must be used until follow-up semen testing confirms that sperm are no longer present.
Yes, vasectomy should be considered a permanent form of birth control. Reversal are often successful, but not always. And reversal is more complex and costly than the original procedure. Men who are unsure about future children should think carefully before scheduling.
A vasectomy reversal may be possible, but success is not guaranteed. Pregnancy after reversal depends on several factors, including time since vasectomy, reproductive health, and partner fertility. VasWeb offers reversal services, but patients should still approach vasectomy as a permanent decision.
Vasectomy does not lower testosterone. Most men report no change in sex drive, erections, or climax sensation. When there is a change, it is more commonly for the better, probably because there is no more worry about unwanted pregnancy. The procedure blocks sperm from entering semen, but it does not interfere with the hormones or physical functions responsible for sexual performance.
Most patients do not notice a visible change in semen after vasectomy. Sperm make up only a small portion of semen volume. After the procedure, the body continues to produce sperm, but sperm can no longer pass into the semen and are naturally absorbed by the body.
Vasectomy is one of the most effective long-term birth control methods, but it is not immediate. The procedure is considered successful only after follow-up semen testing confirms that sperm are absent or below the accepted threshold. Until then, another form of contraception is required.
Most men experience temporary soreness. Some will experience mild swelling and some bruising (discoloration of the skin). Internal bleeding can very rarely cause a blood clot within the scrotum ranging in size from small (like a grape) to large (like a walnut). Even larger clots may require drainage in an operating room but this occurs in fewer than 1 in 200 men. Infection is also extremely rare and usually respond to antibiotics. A lump (sperm granuloma) may develop at the vasectomy site, but usually requires no treatment and acually improves the prognosis for reversal. Prolonged periodic discomfort - known as Post Vasectomy Pain Syndrome when severe - can, on rare occations, require periodic therapy or even a subsequent procedure. Failure occurs in fewer than one in 2000 men. VasWeb explains these risks before treatment so patients can make an informed decision.
VasWeb’s main office is in Tampa/Lutz, and the team also serves patients through multiple clinic locations across Central Florida and surrounding areas, including Orlando, Cocoa, Kissimmee, Ocala, and Port Orange. Patients can review the schedule page to choose a location and date.
Many patients can complete consultation and procedure in one visit after reviewing VasWeb’s online information and counseling video. Patients who want to meet the doctor first can schedule an office visit. Men in their 20s without children are encouraged to discuss the decision before proceeding.
VasWeb's official fee for vasectomy is $690, much less for men with insurance plans with whom we are contracted providers (many plans under Blue Cross, United, Cigna, and Aetna). Men who qualify for Title X federal assistance pay NOTHING! Patients should review payment information before scheduling and call the office with coverage questions.